Menopause is defined as cessation of menstruation for 1 year. The average age of menopause in Asian women is 46 years. With increasing life expectancy, a healthy 50-year-old woman today spends as much as 40% of her life in postmenopausal state. During this prolonged period, women are vulnerable to various conditions, of which one of prime importance and sincere concern is postmenopausal bleeding (PMB). PMB is bleeding that occurs after one year of amenorrhoea in a woman who is not taking hormone replacement therapy. However it is recommended that any vaginal bleeding that occurs six months after the last period (presumed menopause) should be investigated.


PMB occurs in approximately 3 % of post menopausal women. Contributory factors are perhaps increasing awareness, longevity, obesity and hormone therapy both supervised and unsupervised. Abnormal bleeding noted in the genital area is usually attributed to an intrauterine source, but may actually arise from the cervix, vagina, vulva, or fallopian tubes, or be related to ovarian pathology. The origin of bleeding can also involve non gynaecologic sites, such as the urethra, bladder, and rectum/bowel. The differential diagnosis of bleeding in postmenopausal women is less broad than that for abnormal bleeding in premenopausal women and can be enumerated as follows:
Benign conditions represent the most frequent cause of PMB and can cause considerable distress, so most patients will require investigations that explains their symptoms and reassure them that all reasonable assessments have been done.

The aim of assessment and investigation of postmenopausal bleeding is to identify a cause and exclude cancer. Assessment should start by taking a detailed history, with identification of risk factors for endometrial cancer, as well as a medication history covering use of HRT, tamoxifen and anticoagulants. Abdominal and pelvic examinations should be carried out to look for masses. Speculum examination should be performed to see if a source of bleeding can be identified, assess atrophic changes in the vagina and look for evidence of cervical malignancy or polyps. Pap smear is the first and foremost investigation to rule out abnormal cervical or endometrial pathology. This should be followed by detailed endometrial evaluation if required.
The principal diagnostic tools used in the evaluation of endometrium include, endometrial biopsy, dilatation and curettage, ultrasonography and hysteroscopy.
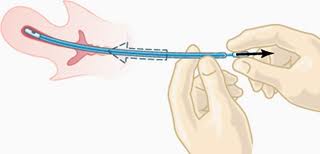
Endometrial biopsy is a simple, outpatient but blind technique employed for obtaining endometrial tissue for histological evaluation. Pipelle/ Vabra aspirator/ Novac's curette can be used with almost 99% sensitivity, low complication rate, and low cost. However, structural abnormalities, such as polyp can be missed, as the cavity cannot be visualised.
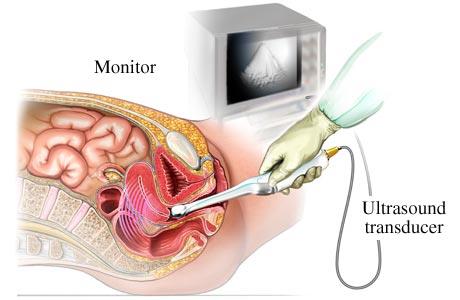
Transvaginal ultrasound examination is an acceptable alternative initial test in postmenopausal women who cannot tolerate office biopsy or it was unsuccessful due to cervical stenosis and in women in whom evaluation of the adnexa or myometrium is indicated. Identification of a regular endometrial echo and the use of a 5mm threshold to define abnormal endometrial thickening effectively excluded abnormalities in post-menopausal patients. However the diagnostic accuracy varies as it is an operator dependant technique.
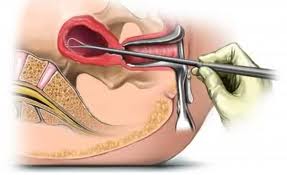
D&C was considered to be the principal diagnostic tool before introduction of hysteroscopy. However, the procedure is blind like endometrial biopsy, and also requires general anaesthesia. There is a risk of uterine perforation and bleeding with the procedure. A study has shown that D&C missed 58% of polyps, 60% of atypical hyperplasia and 11% of endometrial carcinomas.
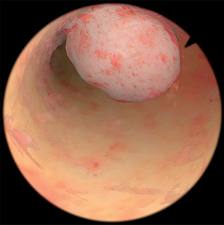
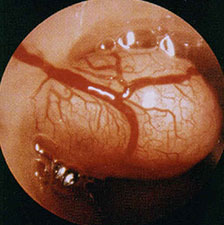
Hysteroscopy is now considered the gold standard for evaluation of endometrial pathology. Advantageously in some instances it can be simultaneously used to treat few benign disorders. Diagnostic hysteroscopy can be done in office settings without the need of any kind of anaesthesia, using new small diameter scopes, with minimal discomfort to the patient. A satisfactory view of the cavity is obtained in more than 90% of cases. Though there is a slight risk of dissemination of endometrial cancer cells and increase chances of positive peritoneal cytology with hysteroscopy, but the viability of these cells is questionable. Low pressure hysteroscopy has been considered to be safe.
In postmenopausal women, uterine bleeding is usually light and self-limited. Exclusion of endometrial cancer is the main objective; therefore, treatment is usually unnecessary once malignancy or premalignant histology has been excluded.
If the examination is normal, the bleeding has stopped and the endometrial thickness is < 5 mm on transvaginal ultrasound scan, no further action need to be taken. Further diagnostic evaluation is indicated for recurrent or persistent bleeding. If a benign lesion is discovered and if the symptoms are bothersome, it should be treated, as appropriate. Local estrogen cream can be used for atrophic endometrium or vaginitis. Benign polyps can be removed hysteroscopically. If a malignancy is diagnosed, surgery is the main stay of treatment. Surgical staging is performed by an exploratory laparotomy, total hysterectomy, bilateral salpingo-oophorectomy, and cytology. Para-aortic and pelvic lymphnode sampling is performed unless there is grade 1 cancer with less than half myometrial invasion. The depth of myometrial invasion is determined by intraoperative frozen section. Subsequent treatment with radiation or chemotherapy depends on the stage of the endometrial tumor.
Five year survival rate for stage I endometrial cancer is almost 98%. Hence it is very important to exclude and treat malignancy. Early diagnosis and prompt treatment is the key to success.